

PED-Antibiotic Tips
PED-Antibiotic Tips
Cavitary Pneumonia / Necrotizing Pneumonia

A well appearing 15yro male has been admitted in our ward for a right lobe lung cavity of about 5cm, one day of fever and chest pain. White Blood Cell count was normal, CRP 75 (normal under 5).
X-ray showed here.
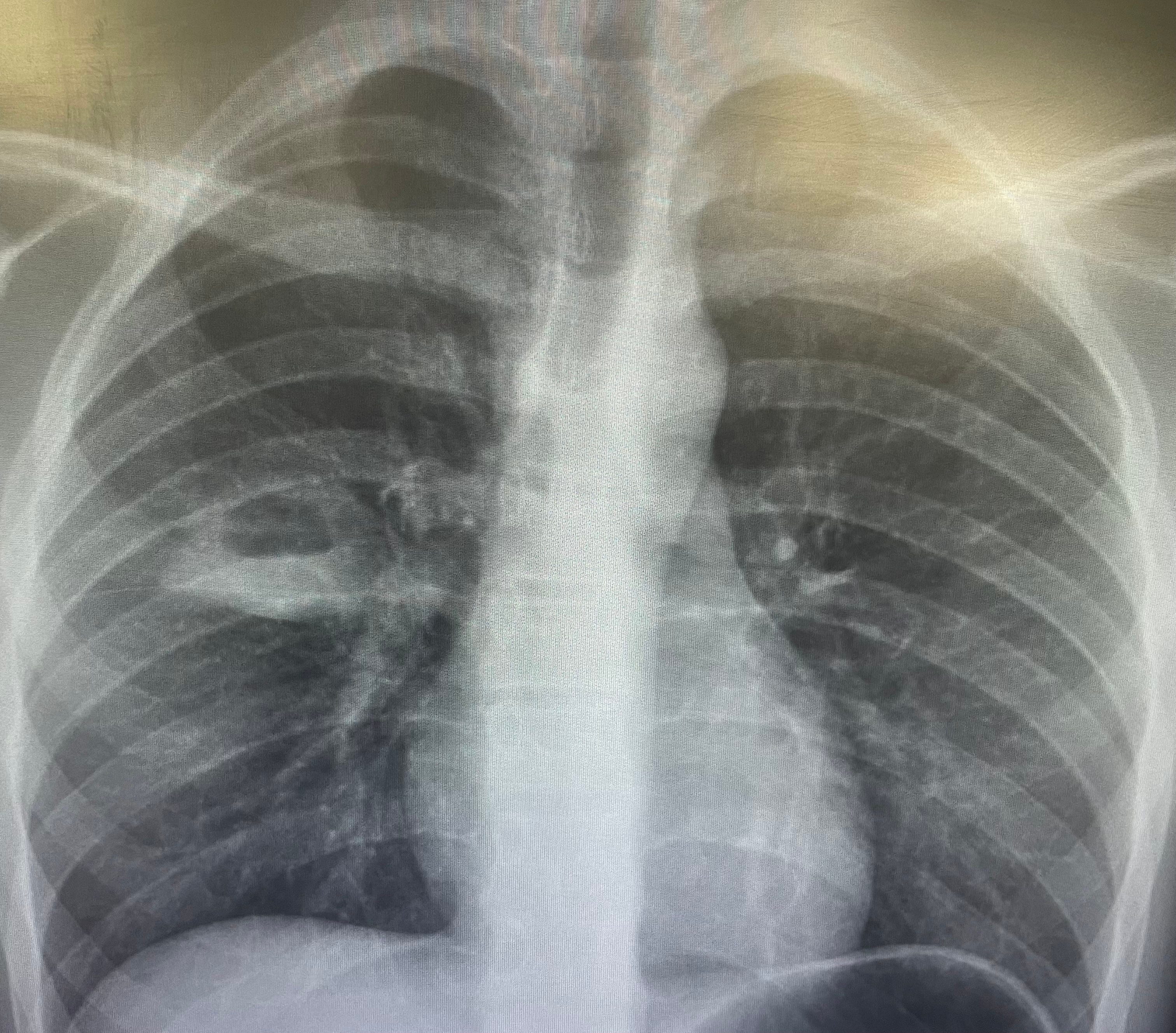
No history of TB contacts nor travels, mantoux and quantiferon negative, BAL negative for M. tuberculosis and bacteria.
Which antibiotic would you chose?
.
.
.
.
.
.
The most common pathogens associated with NP in children are pneumococci and S. aureus.
In addition to pneumococci and S. aureus, other respiratory bacterial and fungal pathogens reported occasionally in studies included in the present review are Streptococcus pyogenes; members of the S. anginosus group; Haemophilus influenzae; Pseudomonas aeruginosa; Stenotrophomonas maltophilia; the anaerobic organism Fusobacterium nucleatum; Mycoplasma pneumoniae; Legionella pneumophila; and Aspergillus species. Unlike in adults, Klebsiella pneumoniae is not a common cause of NP in children,
So, those pathogens should be covered. In Italy, there is a growing incidence of MRSA, so this might be empirically covered. However, MRSA infections (particularly if assocaited with lung cavitations (necrosis) cause severe infections, and are frequently associated with strains expressing the virulence factor Panton-Valentine leukocidin (PVL). In this case, in my opinion that was less probable.
Therefore, I started with IV amoxi/clav.
Do you agree?
.
.
.
.
.
.
I know for sure that most pediatricians (at least in Italy) would start this case iwth ceftriaxone, or, even worse, with Linezolid (as it has great lung penetration and also MRSA coverage). According to the AWARE book of the WHO, Linezolid is part of the antibiotic cathegory “RESERVE”, so it should be used as a reserved option for severe cases without other options. In most other countries, complicated pneumonias (like this) would be treated with amoxiclav, while non-complicated pneumonia would be treated with amoxicillin alone.
Amoxicillin-clavulanate is a combination that offers broader coverage by combining amoxicillin, a penicillin derivative effective against gram-positive and gram-negative bacteria, with clavulanic acid, which counteracts β-lactamase–producing strains.
Antimicrobial Spectrum:
Staphylococcus aureus (methicillin susceptible), Coagulase negative Staphylococci, Streptococcus pneumoniae (penicillin susceptible), Streptococcus spp., Haemophilus influenzae, Moraxella catarrhalis, Neisseria meningitides, Neisseria gonorrhoeae, Enterobacteriaceae, E. coli
Mechanism of Action:
The beta-lactamase inhibitors are recognized as substrates for the beta-lactamases produced by bacteria. This allows the actual beta-lactams to attack the bacterial cell wall by binding to penicillin binding proteins
Pharmacodynamics:
Time dependent killer (Time > MIC)
Do not forget that amoxiclav has a time-dependent action so it is important the time that the grug concentration is above the MIC, and therefore for lung infections is better to give three times a day, giving the drug more time being above the MIC.
How long would you treat this case?
.
.
.
.
.
.
I have treated with a three weeks course of oral amoxiclav, shifted to oral after 3-5 days of IV therapy (the time I needed to exclude TB with BAL) and showed resolution of fever and reduction of CRP from 75 to 25.
The optimal duration for antibiotic treatment of NP is unknown. The median length of antibiotic courses in different studies range from 13 to 42 days, with a median antibiotic course duration of 28 days. Switching from IV to oral antibiotics is appropriate once the child is afebrile for at least 24 h and no longer showing signs of sepsis, their respiratory distress is resolving, enteral feeds are being tolerated, and inflammatory markers are declining. At this point antibiotics are continued for at least another 10–14 days, a recommendation that aligns with consensus guidelines for PPE and empyema complicating pediatric CAP.
If you liked it share and subscribe!
Macrolide ?
Hi. I have managed a number of adults in South Africa in a primary health care clinic with 6 weeks of oral Augmentin(Amoxicillin Clavulanic). We do a chest X-ray at the end to confirm resolution- usually good. Rarely we need to extend a few weeks.